



PANDEMIC ACCORD - Negotiations stall. Failure to reach agreement.
PABS halted the INB negotiations on the Pandemic Accord. Here's why.

“No country in the world that is a low- or middle-income country is going to have enough power to get equitable access,” Matthew Kavanaugh, Director of Georgetown University’s Center for Global Health Policy and Politics
Dear Friend of Global Health Conversations,
Another fortnight - and what’s happened with the Negotiations on the Pandemic Accord? Well, ultimately member states were not able to reach consensus and no treaty will be presented this week. Tonight’s FiRs focus on the outcomes & contentions of the negotiations focussing on Pathogen Access & Benefit sharing. Skip to the Fortnight in Resources below for this.
Greetings, by the way, from the South of France! I’ve had an exciting weekend at the Formula 1 Grand Prix in Monaco 🏎️. As I make my way back to Geneva, I’m looking forward to the important fortnight that lies ahead of us with the commencement of the 77th World Health Assembly. This past week was also the WHO Executive Board PBAC. And while the Pandemic Treaty is not yet finalised, it looks like the WHO International Health Regulations (IHR) Working group should be concluding fairly soon - with 17 out of the 34 amendments to the 2005 version fully approved by member states. (read more)
The bonus podcast episode on the Real Water Scandal is still pending and will be ready during the fortnight. If you subscribe to Global Health Conversations wherever you listen (Spotify, Apple Podcasts, Audible, etc.), you’ll be notified when that episode and the following, The Profitability of Skinny, are released. In the latter I deep-dive on the boom in drugs for diabetes and weight loss management - some of which we discussed in last fortnight’s Q1 Financials and last summer’s ‘Skinny at all costs? Unravelling the weight loss sensation causing supply chain mayhem for Diabetes Type II patients.’
Alongside ongoing reading, I’ve been on William Booth’s 'In Darkest England and the Way Out’. Booth, founder of The Salvation Army, details the diseases that ravaged 1890’s England’s poor communities leading to DALYs, premature death and outbreaks of cholera, typhoid, and tuberculosis. The assumption that underpins everything that we do in this space is the concept that every life is inherently valuable. And I appreciated this quality and assumption within the commentary; making it unique for its era and region. Let us not forget this central assumption - the inherent value of every human life; regardless of where they live, how they live and their ability to pay.
Sending warmth and best wishes,
Christiana

NO AGREEMENT REACHED: The Current State of INB Negotiations on Pathogen Access and Benefit Sharing (PABS) – Article 12
When I started writing this summary earlier in the week, the negotiations were set to conclude on 24 May. Keeping up with the last days of the negotiations; on Friday night it became clear that an agreement would not be reached. The sticking point? PABS. While some areas were agreed, quite a few were not. Specifically under Pathogen Access & Benefit Sharing. Of particular concern were particular obligations on rapid sharing of pathogen material and genetic sequence information. A primary interest area of a number of developed countries was to have such access outside the framework of the Nagoya Protocol on Access to Genetic Resources and the fair and equitable sharing of benefits arising from their utilization through a specialized WHO instrument (such as the PABS system).
I am focussing on this part of the negotiations as, indeed, it is this critical juncture around PABS that brought talks to a standstill. Read the most recent draft here.
Pathogen Access and Benefit Sharing (PABS) here refers to the mechanism through which countries share biological samples of pathogens, such as viruses and bacteria, and the benefits derived from the use of these samples. Benefits can include the development of vaccines, therapeutics, diagnostic tools, and other health-related technologies which could extend to other systems and intelligence related applications such as those that lend themselves to enhancing surveillance systems. PABS is crucial for global health security as it ensures timely access to pathogens for research and the equitable distribution of benefits derived from them. This system is intended to promote equity, particularly ensuring that countries contributing pathogens also receive fair benefits from the resultant medical advancements. In a nutshell: the benefits can be very lucrative.
Over the past days, efforts have been made to bridge gaps between differing national positions on PABS, particularly between high-income countries and low- and middle-income countries including a notable bloc of African nations.
I have a segment on what I have called ‘peripheral controversies’ below. But permit me to introduce these examples (here, here, here) to illustrate why one of the schisms that arose was between low- and middle income countries; and high income countries. This is a big side note - so skip to the next section bold subheading if you only want to read about PABS (Read: How Big Pharma kept COVID-19 vaccine negotiations in South Africa secret)
The culture of mistrust started somewhere. During the COVID-19 pandemic, multinational drug companies imposed stringent terms on South African government negotiations for vaccine access, revealed by newly released confidential contracts and documents. Moderna (initially attempting to charge South Africa $42 / vial in early 2021, four times as much as other suppliers) prohibited disclosure of negotiation details, while Pfizer resisted accountability for delivery issues and transparency in agreements. South Africa paid significantly more for vaccines compared to the European Union, including $10 per Pfizer dose versus the African Union’s $6.75. These revelations highlight Pharma’s leverage in dictating terms. South African officials tried but failed to negotiate better terms due to the concentrated power of the drug companies. Pfizer’s contract included clauses preventing the resale or donation of vaccines without company permission. South Africa paid more for some vaccines than wealthier nations, with Serum Institute’s AstraZeneca doses costing 2.5 times more than the EU's price.
[Afrigen] in Cape Town relied on publicly available information about the Moderna vaccine to develop its own version of a COVID-19 immunization. But there is still concern that the pharmaceutical company will exercise its patents in South Africa, which cover all mRNA vaccine production in the country.
This is all very much beside the point. But these powerful revelations released on Thursday, among others, underscore just how important transparency, trust and clarity around expectations in data sharing is; particularly during a crisis. There is a need for a global solution to create balance and ensure fair access to medical products alongside favourable returns. And without drifting too far from the point at hand, it might be observed that greater transparency will only improve the argument in favour of voluntary licensing. LMICs face a different set of challenges in the effort to secure health equity for populations. Further nuance – middle income countries such as South Africa or Colombia who recently used a compulsory license to procure dolutegravir from ViiV healthcare in order to meet demand – often face a different struggle that is very difficult to navigate. All of the above instances serve to worsen sentiment and trust between private and public sectors. A dedicated instrument, agreed upon, designed to ensure transparency about intellectual property and make data available on something resembling equal footing could possibly allow this trust to rebuild itself.
Draft Negotiating Text and Contentions
The current draft version of the proposed negotiating text for the Pandemic Agreement also lacks reference to a dedicated fund for implementing new obligations related to pandemic prevention, preparedness, and response (a.k.a PPPR). Previous versions had articulated such a fund to finance these obligations. Additionally, this draft merges provisions on technology transfer with sustainable production and consolidates language on compensation and liability management with supply chain and procurement. It importantly presents a streamlined version of the PABS provision without binding benefit-sharing commitments, deferring final modalities to… well, last Friday. But now we’ll have to see. The prediction from yours truly is that the Assembly will conclude that negotiations should resume and continue after the 77th World Health Assembly in the hope of seeking consensus in the months that follow. Ultimately, some compromises will be made.
The key contentious elements in the PABS discussion include the scope of shared information, accountability and traceability, intellectual property, and mandatory financial contributions.
Developing countries have pushed for more specific pathogen-related information, while developed countries have expressed preference for a broader approach. Proposals for tracking users of pathogen information, including registration and traceability, face resistance, too. Debates over IP rights on products developed from shared pathogen information, with many developing countries opposing IP protections. Developing countries have advocated for mandatory monetary contributions and non-monetary benefits like real-time production contributions.
I have had a chance to have a look at the Annex text that is to be presented to the Assembly for consideration as the outcome from the negotiations. It will be accompanied by a separate file entitled ‘Draft text reflecting progress up to FRIDAY 24 May at 12:00 CEST’ which will be integrated. I have not had a chance to read the latter as it is not available at the time of writing, but I’m including the name so that you can easily google it.
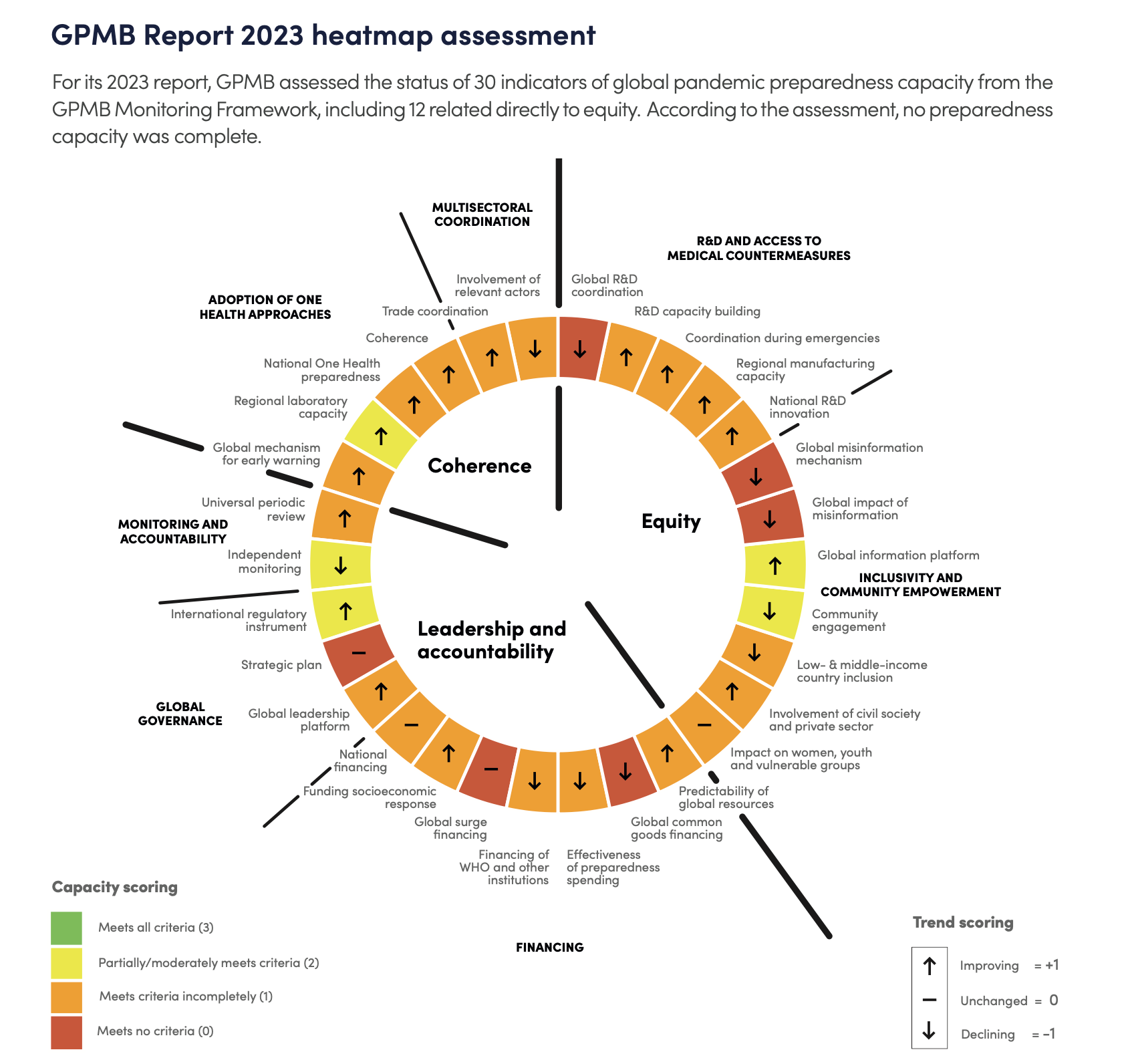
It has been proposed that what is necessary is a PABS system that imposes binding obligations on users of biological materials and genetic sequence data (GSD) to make mandatory monetary contributions. This is seen as essential for ensuring equity, though it is recognized that PABS alone is insufficient without additional measures such as intellectual property waivers and technology transfers. As it is, the Africa Group and the Equity Group are unlikely to agree to a treaty without a strong PABS system. While the pharmaceutical industry is beginning to accept PABS, they prefer access without benefit-sharing obligations, a stance that is widely rejected. This Thursday, the WHO Global Preparedness Monitoring Board released a document entitled Equity in Pandemic Preparedness. The document emphasizes equitable access to medical countermeasures and benefit sharing in pandemic preparedness. Highlighting the fact that during COVID-19, wealthier nations secured vaccines and tests first, leaving low- and middle-income countries and disadvantaged communities behind, enabling repeated infection waves. Prioritizing equity in access and benefit-sharing is essential for effective pandemic management, preventing exacerbation of inequalities, and promoting trust and cooperation
Peripheral Controversies
This past week has also not been free of ‘peripheral controversies’. On Tuesday May 21st, a fake advisory, purported to have been written by President Ramaphosa of South Africa, also current AU COVID-19 Champion, circulated. The document laid out priorities for African countries. As it turned out, this document was not issued by the presidency of the government of South Africa. By Wednesday, it had already been widely disseminated.
Nevertheless, one thing that is true on political dynamics is that differences of opinion across developing countries, such as within the African Group, with some countries aligning with a proposal supported by the EU and the U.S; has added yet another level of political complexity. The latter group presented a revised proposal for Article 12 on PABS, which was debated right until the end of the week. This split is very significant because the African group is known for being very good at cross aligning and reaching a unified stance to include, and with a view to benefit, most of the continent through political solidarity.
Second big one, protests around Geneva – notably small from what I saw – but with a loud online presence. The misinformation about the Pandemic accord, and its aims has been pretty harmful – people who have believed the misinformation have been rightly outraged. Signing petitions and sharing further misinformation.
I was surprised to see major mainstream publications such as the UK’s Telegraph and Newsweek publishing pretty anti-agreement sentiments and quoting people who truly have no business being quoted on such an important topic. According to Nesweek: “WHO is, in reality, asking for a blank check”. This is false. It is important to remember that while the WHO facilitates these discussions, they are in fact being negotiated by member states. Read more about the issues on this point here. The Global Progress Monitoring Board’s paper mentioned earlier also evaluated the progress of the development of a ‘Global misinformation mechanism’ and We have before us an opportunity to create a framework, through our nationally elected officials, to act as a roadmap and guide in the case that there were ever another pandemic threat. I wonder if survivor’s bias makes this concept feel more nebulous, but health security and equity are vitally important. And IMO, there are some people who just need to chill.
Implications of Potential Outcomes – the long shadow of COVID-19
Never again – it’s one of those concepts that has lingered over discussions from the start. The fact that such incredible inequity occurred during COVID-19 in terms of access, IP, discriminatory pricing practices, political moves (such as this & this RE China & Taiwan) countries being essentially penalised for timely sharing of pathogen data (such as this from South Africa).
Thus, many of the member states are approaching discussions with the sentiment that a successful PABS system that centres equity and would ensure that all countries, regardless of GDP, have timely access to pathogen samples and the resultant health benefits. This would reduce disparities in health outcomes and foster trust and collaboration among nations.
The tech transfer & building piece would enable countries to better respond to future health emergencies independently and contribute more actively to global health research. For HICs, a streamlined and efficient PABS system could facilitate faster access to pathogens, accelerating research and development of vaccines and treatments, leading to more rapid containment of pandemics, and so on. Negotiation outcomes will also have a huge influence on global economic and political dynamics. Equitable benefit sharing is hoped to reduce economic disparities and enhance political stability in LMICs. The feeling is that this is one of many steps that would eventually begin to redress the power imbalance that countries experienced two, three and four years ago: countries growing their technological and scientific capabilities. The final agreement will likely establish new legal and ethical frameworks for pathogen sharing. These frameworks will need to balance the interests of protecting public health, respecting national sovereignty and vitally, ensuring fair economic returns from medical innovations.
Ensuring a fair and effective PABS system is not only a matter of justice but also a pragmatic necessity for preparing for future pandemics and safeguarding global health.
Behind the scenes:
One of the highlight’s of my fortnight was organising and hosting a UCL Alumni event and panel in Geneva at Pages & Sips - English bookhop in the Geneva old town. What a special community. This was followed by a lovely, long Pentecost break; some dedicated workspace time and finally, an exciting weekend at the Grand Prix.

Recent Episodes: In case you missed them! 💃🏾
Recent Episodes: In case you missed them! 💃🏾
Episode 19: Drug Licensing and the Pandemic Accord
In this episode, we look at Colombia's recent move in issuing its first compulsory license. The country challenged ViiV Healthcare's monopoly on their patented drug, dolutegravir, an HIV therapeutic, in an attempt to open doors for affordable generic versions and thus improve accessibility & affordability.
Episode 17: PART 1: Dental Dialogue: Prioritising Oral Health in Public Health (ft. Ema Prohić)
& Episode 18: PART 2: Dental Dialogue: Prioritising Oral Health in Public Health (ft. Ema Prohić) - Part 2
Ema and I discuss oral health as a public health issue. Discussing system challenges, incentivisation and disincentivasation, dental caries as the most common infectious disease, bacteria and the use of antibiotics. We also discuss a public health project that I led back in 2020 with the Ministry of Health Qatar and PHCC wherein she focussed on integrating oral health into a primary care program. Ema is a doctor of dental medicine from Croatia, currently undertaking her specialization in orthodontics and facial orthopedics in Barcelona as well as working in the UK in several dental practices as an NHS and private practitioner.